
9 Cholesterol Myths That Keep Your Blood Pressure High (Vascular Surgeons Reveal the Real Culprit)
Your doctor says your cholesterol is high. You cut out eggs, switch to low-fat everything, and pop a statin daily. But here’s what most people don’t know: while you’re obsessing over cholesterol numbers, chronic inflammation might be silently building dangerous plaque in your arteries, regardless of your cholesterol levels.
If you’re confused by contradictory cholesterol advice and unaware that insulin resistance and metabolic dysfunction actually drive arterial plaque formation, you’re missing the bigger picture of vascular health.
You’ll discover why cholesterol alone doesn’t tell the full story, how chronic inflammation actually builds plaque in your arteries, the surprising role of metabolic syndrome, and science-backed strategies that address root causes instead of just chasing numbers.
Artery Weather
The Real Villain
Cholesterol isn’t the enemy. It’s the building block for cells. The real storm is inflammation, which damages artery walls and traps LDL.
The Truth About Cholesterol: Why Inflammation, Not Just High Numbers, Builds Arterial Plaque
Your doctor looks at your cholesterol numbers and frowns. You leave with a prescription and a list of foods to avoid. But here's what most people don't know: cholesterol isn't the villain you think it is. The real problem hiding in your arteries has nothing to do with that number on your lab report.
For decades, we've been told the same story. High cholesterol clogs your arteries like grease in a pipe. Lower the number, save your heart. Simple, right? Wrong. New research in 2025 shows the truth is far more interesting—and helpful. Understanding what actually builds plaque in your arteries can save your life.
Myth #1: Cholesterol Is the Enemy—Cut It Out Completely

Your body needs cholesterol to survive. Every cell in your body uses it to build strong walls. Your brain runs on it. It makes hormones that control everything from stress to sleep. Without cholesterol, you'd die.
The problem isn't cholesterol itself. It's what happens when LDL cholesterol gets damaged by inflammation. Think of it like fruit sitting on your counter. Fresh fruit is healthy. But when it sits too long and starts to rot, it becomes a problem. LDL works the same way.
Key Points:
- Your body makes vitamin D from cholesterol when sunlight hits your skin
- LDL only becomes dangerous when it gets oxidized and combines with inflammation in your artery walls
- A 2025 study tracked 100 lean, healthy people eating ketogenic diets with high LDL—they showed no plaque buildup
- The apoB test predicts heart risk better than LDL numbers alone, according to Harvard Health research
- Inflammation markers like CRP and IL-6 tell you more about your heart risk than your cholesterol number
Context matters more than the number on your lab sheet. A metabolically healthy person with high LDL might be fine. Someone with lower LDL but high inflammation could be in serious trouble. This changes everything we thought we knew.
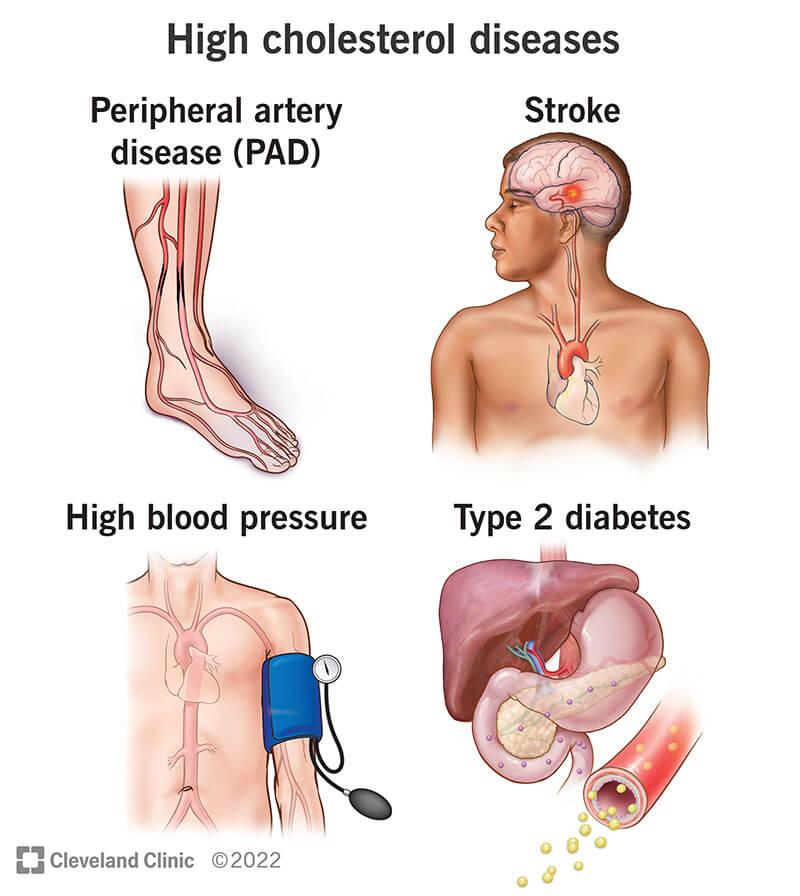
Myth #2: High Cholesterol Automatically Raises Blood Pressure
Here's what happens at most doctor visits. High cholesterol? Check. High blood pressure? Check. The doctor assumes they're connected. But cholesterol doesn't directly cause high blood pressure. These are two separate problems that often show up together.
Over 60% of people with high blood pressure also have high cholesterol. That sounds connected, right? But correlation isn't causation. Both problems share the same root causes: inflammation, insulin resistance, and damage to your blood vessel walls.
Key Points:
- About 40% of American adults have high cholesterol, while nearly 48% have high blood pressure
- You can have high cholesterol without cardiovascular disease, and vice versa
- Endothelial dysfunction (damage to blood vessel walls) drives both problems
- Insulin resistance creates a cascade that affects both cholesterol and blood pressure
- Chronic inflammation links the two conditions, but cholesterol doesn't cause blood pressure to rise directly
The connection exists, but it's indirect. Think of inflammation as the fire. High cholesterol and high blood pressure are both smoke. Treating the smoke won't put out the fire. You need to find what's burning.
Myth #3: Thin People Don't Need to Worry About Cholesterol

Walk into any gym and you'll see thin people assuming they're safe from heart disease. Body weight doesn't tell the whole story. You can be slim and still have dangerous plaque building in your arteries.
Genetics plays a massive role. Familial hypercholesterolemia affects 1 in 200 people, causing sky-high cholesterol regardless of diet or weight. Then there's the "skinny fat" problem—people who look thin but carry dangerous visceral fat around their organs. This fat acts differently than the fat you can see.
Key Points:
- Normal-weight metabolically obese (NWMO) phenotype describes thin people with metabolic problems
- Visceral fat surrounds your organs and releases inflammatory chemicals, while subcutaneous fat sits under your skin and causes fewer problems
- Insulin resistance can develop in thin people, especially with poor diet and lack of exercise
- Metabolic health matters more than BMI when predicting heart disease risk
- Some thin people have more dangerous fat distribution than overweight individuals with healthy metabolic markers
Your mirror can't show you insulin resistance. It can't reveal inflammation burning in your arteries. A thin person eating processed foods and sitting all day might have worse arterial health than someone heavier who exercises and eats real food.
Myth #4: Cholesterol Is the Only Plaque-Building Culprit
This is where everything changes. Atherosclerosis isn't a cholesterol disease. It's a chronic inflammatory disease that happens at sites where blood flow gets disturbed. Russell Ross first proposed this in 1999, and decades of research have proven him right.
Here's what actually happens in your arteries. First, something damages the endothelium (the thin layer of cells lining your blood vessels). This damage could come from high blood sugar, smoking, stress, or inflammatory foods.
Once damaged, your immune system sends white blood cells to investigate. These cells slip into the artery wall where they don't belong.
Key Points:
- Pro-inflammatory stimuli cause endothelial dysfunction, allowing immune cells and lipoproteins to migrate into the arterial wall
- LDL must be oxidized before macrophages (white blood cells) can uptake it to form foam cells
- Foam cells are bloated immune cells stuffed with oxidized LDL—they're the building blocks of plaque
- Inflammatory cells release matrix metalloproteinases that destroy the fibrous cap holding plaque stable, leading to vulnerable plaques that can rupture
- Oxidative stress and ROS (reactive oxygen species) production drive the inflammation cycle
The sequence matters: endothelial damage happens first, then monocyte infiltration, then foam cell formation, then plaque buildup. Cholesterol is just one player in a complex inflammatory process.
Myth #5: You'll Feel It When Your Cholesterol Is High

You won't feel high cholesterol building up. No warning signs. No pain. No fatigue. This silent process happens over decades while you go about your normal life. By the time you feel something, you're having a heart attack or stroke.
The only visible symptom of extremely high cholesterol is rare: xanthomas. These are yellowish, cholesterol-rich deposits that show up on your skin, usually around your eyes or on your hands. Most people never get them. Similarly, inflammation and plaque buildup work in secret, destroying your arteries with zero symptoms.
Key Points:
- The CDC recommends getting your cholesterol checked at least every 5 years, starting at age 20
- Advanced screening options include CAC (coronary artery calcium) scores, apoB testing, and inflammatory marker panels
- Silent plaque buildup can progress for 20-30 years before causing symptoms
- First symptom of heart disease is often a heart attack
- Testing inflammatory markers like CRP reveals problems before plaque becomes dangerous
This is why regular screening saves lives. You can't manage what you don't measure. Waiting until you feel bad is waiting too long. Your arteries could be silently clogging while you feel perfectly fine.
Myth #6: Eating Cholesterol Foods Spikes Your Blood Levels
Eat an egg and your cholesterol spikes, right? Not quite. The relationship between dietary cholesterol and blood cholesterol is far more complex than we thought. Your liver makes most of the cholesterol in your bloodstream. When you eat more cholesterol, your liver makes less. When you eat less, it makes more.
What you eat matters, but not the way you think. Saturated fat and refined carbohydrates have a bigger impact on your blood cholesterol than dietary cholesterol itself. Eating sugars and simple carbs triggers inflammation and spikes insulin, which can result in higher cholesterol levels.
Key Points:
- Your liver produces about 75% of the cholesterol in your blood, while diet contributes only about 25%
- Keep saturated fat to less than 6% of daily calories for heart health
- Refined carbs and sugar trigger insulin resistance and inflammation, raising cholesterol more than dietary cholesterol does
- Individual response varies widely based on genetics and metabolic health
- Some people are "hyper-responders" whose blood cholesterol rises with dietary cholesterol, but most people's levels stay stable
The bigger issue is how your body responds to what you eat. Someone with good insulin sensitivity can handle dietary cholesterol fine. Someone with insulin resistance will see their numbers climb from sugar and processed foods, even if they avoid cholesterol completely.
Myth #7: There's One Target Number That Fits Everyone

Your friend brags about their cholesterol being under 200. Your doctor wants yours below 100. Your neighbor's cardiologist set their target at 70. Who's right? They all might be, depending on individual risk.
Cholesterol targets vary wildly based on your cardiovascular risk, history, and metabolic health. For healthy adults with no risk factors, LDL at or below 100 mg/dL is ideal. For those with heart disease or stroke history, the target drops to 70 mg/dL or lower. Context drives everything.
Key Points:
- The American Heart Association and American College of Cardiology have different guidelines for different risk categories
- 10-year CVD risk calculators help determine your personal target
- Inflammation status, insulin resistance, and family history affect your ideal number
- Someone with high inflammation needs lower LDL than someone with low inflammation
- Metabolic health markers beyond cholesterol (like HbA1c and HOMA-IR) matter just as much
One-size-fits-all medicine doesn't work for cholesterol. A 30-year-old marathon runner with perfect metabolic health can tolerate higher LDL than a 60-year-old diabetic with high inflammation. Your number should be personalized to your risk.
Myth #8: Just Take a Statin and You're Protected
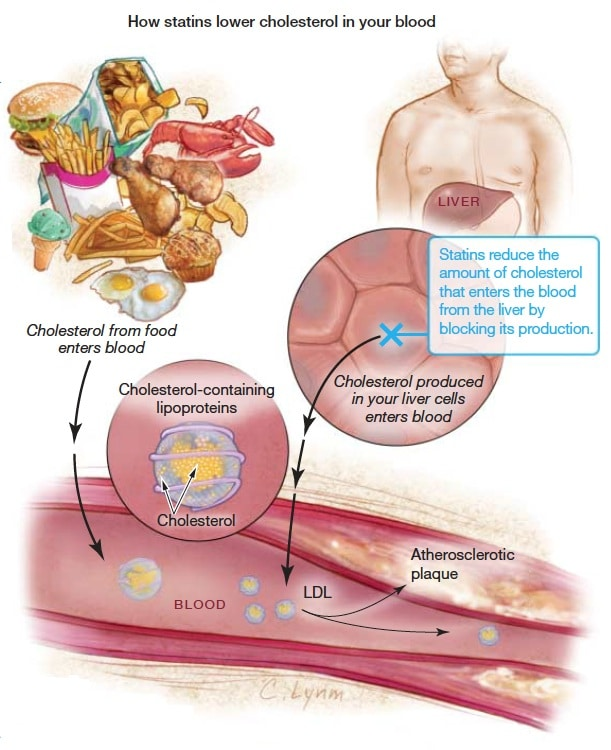
Statins lower LDL cholesterol effectively. They've saved countless lives. But they don't fix the underlying problem. Taking a statin while ignoring insulin resistance and inflammation is like mopping the floor while the sink overflows.
Statins are not weight-reducing drugs. They don't improve your diet. They don't reduce visceral fat. They don't address the metabolic syndrome characterized by visceral obesity, insulin resistance, and chronic inflammation. These root causes require lifestyle intervention, not just medication.
Key Points:
- 150 minutes of moderate-intensity cardio weekly helps lower both cholesterol and blood pressure
- Plant-based diets high in fiber and unsaturated fats show the best results for reducing inflammation
- Mediterranean diet reduces cardiovascular events by 30% in high-risk patients
- Newer therapies like PCSK9 inhibitors and bempedoic acid work differently than statins for people who can't tolerate them
- Omega-3 fatty acids reduce inflammation and can lower triglycerides by 20-30%
Diet, exercise, and stress management address the root causes that statins ignore. Anti-inflammatory strategies matter: eating colorful vegetables, adding omega-3s from fatty fish, exercising regularly, and managing stress. Statins can be part of the solution, but they're not the whole answer.
Myth #9: Heart Disease Is Mainly a Man's Problem

Women get a dangerous message: heart disease is a man's problem. The numbers tell a different story. CDC data from 2015-2018 shows high cholesterol affects 10.5% of men and 12.1% of women. After menopause, women's heart disease risk accelerates to match men's.
More heart attacks are recorded annually in women than men. This happens because women live longer and develop heart disease later in life. But when women have heart attacks, they tend to have worse outcomes. Their symptoms often get missed because they present differently than men's classic chest pain.
Key Points:
- Estrogen provides protective effects before menopause, keeping cholesterol lower and arteries healthier
- After menopause, estrogen drops and heart disease risk rises sharply
- Women often experience atypical heart attack symptoms like fatigue, nausea, and jaw pain instead of chest pain
- Gender differences affect how inflammation and metabolism respond to stress
- Women's heart disease often goes undiagnosed longer because both patients and doctors miss the signs
Heart disease kills more women than all cancers combined. Yet many women still think it won't happen to them. Screening and prevention matter just as much for women as men, especially after age 50.
What Vascular Surgeons Say: The Real Root Cause of Arterial Plaque

Talk to vascular surgeons who see inside arteries every day. They'll tell you the same thing: metabolic syndrome drives the whole process. This syndrome combines chronic low-grade inflammation with insulin resistance, creating a perfect storm in your blood vessels.
Insulin resistance doesn't just affect blood sugar. It causes endothelial dysfunction, increases vascular resistance, and triggers inflammation in vessel walls. Hyperinsulinemia (too much insulin) accelerates atherosclerosis through multiple mechanisms, including smooth muscle proliferation and inflammation activation. Your body stays in a constant state of inflammation.
Key Points:
- Over 1 in 5 Americans and Europeans are affected by metabolic syndrome right now
- Up to 75% of the association between metabolic syndrome and arterial stiffness is mediated by inflammation markers and insulin resistance
- Visceral fat acts as an endocrine organ, releasing inflammatory cytokines like TNF-α, IL-6, and IL-1β
- CRP (C-reactive protein) and fibrinogen are inflammatory markers that predict heart attacks better than cholesterol alone
- The cascade goes: poor diet and stress lead to insulin resistance, which causes chronic inflammation, which damages endothelium, which allows oxidized LDL uptake, which forms plaque
Here's the real sequence. You eat processed foods high in sugar and refined carbs. Your insulin spikes repeatedly. Over time, your cells stop responding to insulin. Your pancreas pumps out more insulin to compensate. This excess insulin damages your blood vessel walls.
Inflammation kicks in to heal the damage, but becomes chronic. Damaged vessel walls let oxidized LDL particles slip inside. Immune cells rush in to clean up. They become foam cells. Plaque forms.
2025 studies show 20-30% plaque reduction is possible through targeted nutrition that addresses inflammation. This isn't theoretical. Real people are reversing arterial damage by fixing their metabolic health.
Evidence-Based Strategies to Reduce Inflammation and Protect Your Arteries
You can't change your genetics, but you can change your metabolic health. Start with insulin resistance. Switch to a low-glycemic diet that doesn't spike your blood sugar. Try intermittent fasting to give your pancreas a break. Add resistance training to build muscle that soaks up glucose.
Reduce chronic inflammation through food choices. The Mediterranean diet works because it's loaded with anti-inflammatory compounds. Add omega-3s from fatty fish. Eat foods rich in polyphenols like berries, dark chocolate, and green tea. Get 7-8 hours of quality sleep. Manage your stress before it becomes chronic.
Key Points:
- Test the right markers: get CRP, apoB, insulin/HOMA-IR, and HbA1c tested beyond your standard lipid panel
- Exercise strategically with both cardio (150 minutes weekly) and resistance training
- Eating diverse polyphenol-rich foods provides long-term heart benefits according to Harvard Health
- Specific foods to add: berries, leafy greens, fatty fish, walnuts, extra virgin olive oil, turmeric
- Consider supplements based on testing: omega-3s (EPA and DHA), vitamin D, B vitamins, magnesium
- Emerging research on nattokinase showed 36% plaque reduction in a 2025 study, though more research is needed
Sleep matters more than most people realize. Poor sleep raises cortisol, which drives inflammation and insulin resistance. Aim for 7-8 hours of quality sleep in a dark, cool room. Manage stress through whatever works for you: meditation, time in nature, exercise, or therapy.
Your arteries respond to what you do every day. One healthy meal won't fix years of damage. But consistent changes add up. Inflammation drops. Insulin sensitivity improves. Your endothelium heals. New plaque stops forming, and existing plaque can stabilize or even shrink.
The Bottom Line: Focus on What Really Matters
Cholesterol myths have distracted us from the real issue for decades. Chronic inflammation and metabolic dysfunction drive arterial plaque formation, not cholesterol numbers alone. Inflammation, not cholesterol by itself, damages your arteries and allows plaque to build.
Insulin resistance and metabolic syndrome are the root causes. They require lifestyle intervention, not just a pill. Testing inflammatory markers and metabolic health matters as much as checking your cholesterol numbers. A comprehensive approach addressing diet, exercise, stress, and sleep works better than obsessing over one number.
Key Points:
- Get tested for inflammatory markers (CRP, apoB) and insulin resistance alongside your cholesterol panel
- Start with one anti-inflammatory dietary change this week
- Swap refined carbs for colorful vegetables at one meal daily
- Add omega-3 rich fish twice weekly
- Move your body for at least 30 minutes most days
- Prioritize sleep and stress management as much as diet
Talk to your doctor about expanding your testing beyond basic cholesterol. Ask for CRP, apoB, HbA1c, and fasting insulin. These markers reveal what's really happening in your arteries. Your cholesterol number tells part of the story. Your metabolic health tells the rest.
Your arteries will thank you for focusing on what actually matters: reducing inflammation, improving insulin sensitivity, and building real metabolic health. The number on your cholesterol test isn't the enemy. Chronic inflammation is. Fix that, and your arteries can heal.






